
Chapter 12: Micronutrients in Bones, Blood, and Eyes
12.9 Vitamin A
University of Hawai‘i at Mānoa Food Science and Human Nutrition Program
Vitamin A Functions and Health Benefits
Vitamin A is a generic term for a group of similar compounds called retinoids. Retinol is the form of vitamin A found in animal-derived foods, and is converted in the body to the biologically active forms of vitamin A: retinal and retinoic acid (thus retinol is sometimes referred to as “preformed vitamin A”). About 10 percent of plant-derived carotenoids, including beta-carotene, can be converted in the body to retinoids and are another source of functional vitamin A. Carotenoids are pigments synthesized by plants that give them their yellow, orange, and red color. Over six hundred carotenoids have been identified and, with just a few exceptions, all are found in the plant kingdom. There are two classes of carotenoids—the xanthophylls, which contain oxygen, and the carotenes, which do not.
In plants, carotenoids absorb light for use in photosynthesis and act as antioxidants. Beta-carotene, alpha-carotene, and beta-cryptoxanthin are converted to some extent to retinol in the body. The other carotenoids, such as lycopene, are not. Many biological actions of carotenoids are attributed to their antioxidant activity, but they likely act by other mechanisms, too.
Vitamin A is fat-soluble and is packaged into chylomicrons in small intestine, and transported to the liver. The liver stores and exports vitamin A as needed; it is released into the blood bound to a retinol-binding protein, which transports it to cells. Carotenoids are not absorbed as well as vitamin A, but similar to vitamin A, they do require fat in the meal for absorption. In intestinal cells, carotenoids are packaged into the lipid-containing chylomicrons inside small intestine mucosal cells and then transported to the liver. In the liver, carotenoids are repackaged into lipoproteins, which transport them to cells.
The retinoids are aptly named as their most notable function is in the retina, the layer of cells at the back of the eye that detect light. The retinoids aid in vision, particularly in seeing under low-light conditions. This is why night blindness is the most definitive sign of vitamin A deficiency. Vitamin A has several important functions in the body, including maintaining vision and a healthy immune system. Many of vitamin A’s functions in the body are similar to the functions of hormones (for example, vitamin A can interact with DNA, causing a change in protein function). Vitamin A assists in maintaining healthy skin and the linings and coverings of tissues; it also regulates growth and development. As an antioxidant, vitamin A protects cellular membranes, helps in maintaining glutathione levels, and influences the amount and activity of enzymes that detoxify free radicals.
Vision
Retinol that is circulating in the blood is taken up by cells in the eye retina, where it is converted to retinal and is used to help the pigment rhodopsin, which is involved in the eye’s ability to see under low light conditions. A deficiency in vitamin A thus results in less rhodopsin and a decrease in the detection of low-level light, a condition referred to as night-blindness.
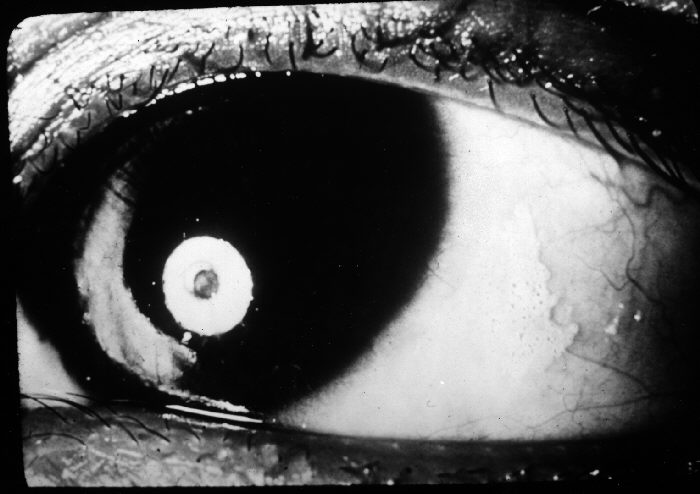
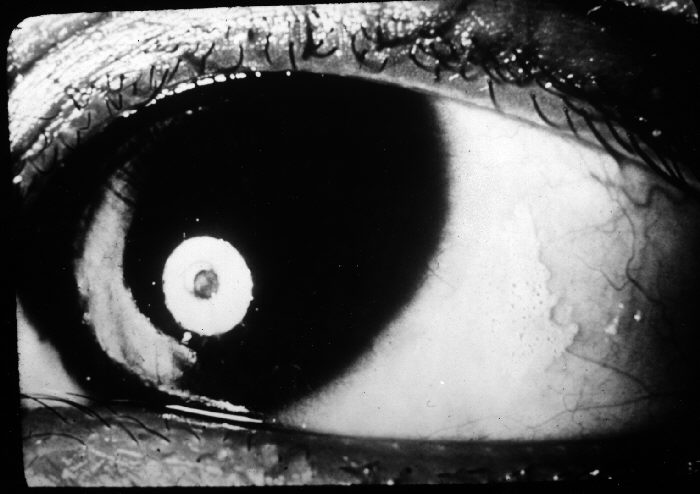
Insufficient intake of dietary vitamin A over time can also cause complete vision loss. In fact, vitamin A deficiency is the number one cause of preventable blindness worldwide. Vitamin A not only supports the vision function of eyes but also maintains the coverings and linings of the eyes. Vitamin A deficiency can lead to the dysfunction of the linings and coverings of the eye (eg. bitot spots), causing dryness of the eyes, a condition called xerophthalmia. The progression of this condition can cause ulceration of the cornea and eventually blindness.
Immunity
The common occurrence of advanced xerophthalmia in children who died from infectious diseases led scientists to hypothesize that supplementing vitamin A in the diet for children with xerophthalmia might reduce disease-related mortality. In Asia in the late 1980s, targeted populations of children were administered vitamin A supplements, and the death rates from measles and diarrhea declined by up to 50 percent. Vitamin A supplementation in these deficient populations did not reduce the number of children who contracted these diseases, but it did decrease the severity of the diseases so that they were no longer fatal. Soon after the results of these studies were communicated to the rest of the world, the World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) commenced worldwide campaigns against vitamin A deficiency. UNICEF estimates that the distribution of over half a billion vitamin A capsules prevents 350,000 childhood deaths annually.[1]
In the twenty-first century, science has demonstrated that vitamin A greatly affects the immune system. What we are still lacking are clinical trials investigating the proper doses of vitamin A required to help ward off infectious disease and how large of an effect vitamin A supplementation has on populations that are not deficient in this vitamin. This brings up one of our common themes in this text—micronutrient deficiencies may contribute to the development, progression, and severity of a disease, but this does not mean that an increased intake of these micronutrients will solely prevent or cure disease. The effect, as usual, is cumulative and depends on the diet as a whole, among other things.
Growth and Development
Vitamin A acts similarly to some hormones in that it is able to change the amount of proteins in cells by interacting with DNA. This is the primary way that vitamin A affects growth and development. Vitamin A deficiency in children is linked to growth retardation; however, vitamin A deficiency is often accompanied by protein malnutrition and iron deficiency, thereby confounding the investigation of vitamin A’s specific effects on growth and development.
In the fetal stages of life, vitamin A is important for limb, heart, eye, and ear development and in both deficiency and excess, vitamin A causes birth defects. Furthermore, both males and females require vitamin A in the diet to effectively reproduce.
Cancer
Vitamin A’s role in regulating cell growth and death, especially in tissues that line and cover organs, suggests it may be effective in treating certain cancers of the lung, neck, and liver. It has been shown in some observational studies that vitamin A-deficient populations have a higher risk for some cancers. However, vitamin A supplements have actually been found to increase the risk of lung cancer in people who are at high risk for the disease (i.e., smokers, ex-smokers, workers exposed to asbestos). The Beta-Carotene and Retinol Efficacy Trial (CARET) involving over eighteen thousand participants who were at high risk for lung cancer found that people who took supplements containing very high doses of vitamin A (25,000 international units) and beta-carotene had a 28 percent higher incidence of lung cancer midway through the study, which was consequently stopped.[2]
Vitamin A Toxicity
Vitamin A toxicity, or hypervitaminosis A, is rare. Typically it requires you to ingest ten times the RDA of preformed vitamin A in the form of supplements (it would be hard to consume such high levels from a regular diet) for a substantial amount of time, although some people may be more susceptible to vitamin A toxicity at lower doses. The signs and symptoms of vitamin A toxicity include dry, itchy skin, loss of appetite, swelling of the brain, and joint pain. In severe cases, vitamin A toxicity may cause liver damage and coma.
Vitamin A is essential during pregnancy, but doses above 3,000 micrograms per day (10,000 international units) have been linked to an increased incidence of birth defects. Pregnant women should check the amount of vitamin A contained in any prenatal or pregnancy multivitamin she is taking to assure the amount is below the UL.
Dietary Reference Intakes for Vitamin A
There is more than one source of vitamin A in the diet. There is preformed vitamin A, which is abundant in many animal-derived foods, and there are carotenoids, which are found in high concentrations in vibrantly colored fruits and vegetables and some oils.
Some carotenoids are converted to retinol in the body by intestinal cells and liver cells. However, only minuscule amounts of certain carotenoids are converted to retinol, meaning fruits and vegetables are not necessarily good sources of vitamin A.
The RDA for vitamin A includes all sources of vitamin A. The RDA for vitamin A is given in mcg of retinol activity requirements (RAE) to take into account the many different forms it is available in. The human body converts all dietary sources of vitamin A into retinol. Therefore, 1 mcg of retinol is equivalent to 12 mcg of beta-carotene, and 24 mcg of alpha-carotene or beta-cryptoxanthin. For example, 12 micrograms of fruit- or vegetable-based beta-carotene will yield 1 microgram of retinol. Currently vitamin A listed in food and on supplement labels use international units (IUs). The following conversions are listed below[3]:
- 1 IU retinol = 0.3 mcg RAE
- 1 IU beta-carotene from dietary supplements = 0.15 mcg RAE
- 1 IU beta-carotene from food = 0.05 mcg RAE
- 1 IU alpha-carotene or beta-cryptoxanthin = 0.025 mcg RAE
The RDA for vitamin A is considered sufficient to support growth and development, reproduction, vision, and immune system function while maintaining adequate stores (good for four months) in the liver.
Table 12.91 Dietary Reference Intakes for Vitamin A[4]
| Age Group | RDA Males and Females (mcg RAE/day) | UL |
| Infants (0–6 months) | 400* | 600 |
| Infants (7–12 months) | 500* | 600 |
| Children (1–3 years) | 300 | 600 |
| Children (4–8 years) | 400 | 900 |
| Children (9–13 years) | 600 | 1,700 |
| Adolescents (14–18 years) | 900 (males), 700 (females) | 2,800 |
| Adults (> 19 years) | 900 (males), 700 (females) | 3,000 |
| Pregnancy | 750 (14-18y), 770 (19-50y) | Same as non-pregnant |
| Lactation | 1,200 (14-18y), 1,300 (19-50y) | Same as non-lactating |
| *denotes Adequate Intake | ||
Dietary Sources of Vitamin A and Beta-Carotene
Preformed vitamin A is found only in foods from animals, with the liver being the richest source because that’s where vitamin A is stored (see Table 12.92 “Vitamin A Content of Various Foods”). The dietary sources of carotenoids will be given in the following text.
Table 12.92 Vitamin A Content of Various Foods[5]
| Food | Serving | Vitamin A (IU) | Percent Daily Value |
| Beef liver | 3 oz. | 27,185 | 545 |
| Chicken liver | 3 oz. | 12,325 | 245 |
| Milk, skim | 1 c. | 500 | 10 |
| Milk, whole | 1 c. | 249 | 5 |
| Cheddar cheese | 1 oz. | 284 | 6 |
In the United States, the most consumed carotenoids are alpha-carotene, beta-carotene, beta-cryptoxanthin, lycopene, lutein, and zeaxanthin. See Table 12.93 “Alpha- and Beta-Carotene Content of Various Foods” for the carotenoid content of various foods.
Table 12.93 Alpha- and Beta-Carotene Content of Various Foods[6]
| Food | Serving | Beta-carotene (mg) | Alpha-carotene (mg) |
| Pumpkin, canned | 1c. | 17.00 | 11.70 |
| Carrot juice | 1c. | 22.00 | 10.20 |
| Carrots, cooked | 1c. | 13.00 | 5.90 |
| Carrots, raw | 1 medium | 5.10 | 2.10 |
| Winter squash, baked | 1c. | 5.70 | 1.40 |
| Collards, cooked | 1c. | 11.60 | 0.20 |
| Tomato | 1 medium | 0.55 | 0.10 |
| Tangerine | 1 medium | 0.13 | 0.09 |
| Peas, cooked | 1c. | 1.20 | 0.09 |
- Sommer A. Vitamin A Deficiency and Clinical Disease: An Historical Overview. J Nutr. 2008; 138, 1835–39. http://jn.nutrition.org/content/138/10/1835.long. Accessed October 4, 2017. ↵
- Goodman GE, et al. The Beta-Carotene and Retinol Efficacy Trial: Incidence of Lung Cancer and Cardiovascular Disease Mortality During 6-year Follow-up after Stopping Beta-Carotene and Retinol Supplements. J Natl Cancer Inst. 2004; 96(23), 1743–50. http://jnci.oxfordjournals.org/content/96/23/1743.long. Accessed October 6, 2017. ↵
- Dietary Supplement Fact Sheet: Vitamin A. National Institutes of Health, Office of Dietary Supplements. http://ods.od.nih.gov/factsheets/VitaminA-QuickFacts/. Updated September 5, 2012. Accessed October 7, 2017. ↵
- Dietary Fact Sheet for Health Professionals: Vitamin A. National Institute of Health, Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminA-HealthProfessional/. Updated June 15, 2022. Accessed August 3, 2023. ↵
- Source: Dietary Supplement Fact Sheet: Vitamin A. National Institutes of Health, Office of Dietary Supplements. http://ods.od.nih.gov/factsheets/VitaminA-QuickFacts/. Updated September 5, 2012. Accessed October 7, 2017. ↵
- Source: 2010. USDA National Nutrient Database for Standard Reference, Release 23. US Department of Agriculture, Agricultural Research Service. http://www.ars.usda.gov/ba/bhnrc/ndl. Accessed October 22, 2017. ↵
The retinoids are a family of compounds that are structurally and functionally similar to vitamin A.
Photosynthesis is the process by which plants use energy from sunlight to convert carbon dioxide gas (CO2) from the atmosphere into sugar molecules, like glucose.
Chylomicrons are lipoproteins formed by the merging of a protein carrier, triglycerides, cholesterol, and phospholipids.
Absorption is the process of getting nutrients from the digestive tract into the blood or lymph.
Free Radical – a molecule with an unpaired electron in its outer orbital. Free radicals are highly reactive because they actively seek an electron to stabilize (pair with) the unpaired electron within the molecule. This makes free radicals very strong oxidants.
Malnutrition refers to one not receiving proper nutrition and does not distinguish between the consequences of too many nutrients or the lack of nutrients, both of which impair overall health.
Pregnancy is the development of a zygote into an embryo and then into a fetus in preparation for childbirth.

{kind=link}
{kind=link}